
I will get to some points about the CDC’s updated masking policy in a moment. But first a few points about the CDC’s decision-making generally. I thought the earlier decision to end the masking guidance for the vaccinated was a mistake. I think the CDC was trying to balance the evolving science with immense public pressure to offer what amounts to a reward for vaccination, to declare the pandemic over or show the benefits of vaccination.
But after yesterday’s updated policy or reversal I kept seeing comments on Twitter, headlines in OpEds and comments from people on TV saying, “That’s it!” “That’s the final nail in the coffin of the CDC’s credibility!” Or ‘the experts’ or Fauci or whoever else. “First it was no masks! Now masks are back! Which is it??!?!!?”
Really people need to get the f*#$ over themselves.
COVID is an evolving pathogen. Our knowledge of it is evolving. We’re basically conducting, against our will, a live subject study with the entire human population. Science isn’t a book with all the answers. It’s an empirical process. By its nature it’s tentative and evolving. We are learning about the efficacy of the best vaccines. We’re learning about Delta COVID. And we’re trying to figure out how the two interact.
This isn’t a brief for anyone at CDC. Like I said, I think they’ve gotten some key decisions wrong, in ways I’ll describe in a moment. Mostly they are not clinical decisions but decisions which have sought to balance the available scientific knowledge with evolving public opinion. Or to be more specific, they are cases where they have sought to balance it with what we might call very understandable public exhaustion.
The fact is that we are living through an historic global pandemic. It’s complicated. We’re collectively having to make big decisions without anywhere near enough knowledge. It will continue to be bumpy. The problem isn’t that the CDC doesn’t have enough wizards to wave wands to make it disappear for you. The problem is the virus. And we are not done with it.
As I suggested above, the real challenges now are balancing the the current scientific knowledge with the political realities of an exhausted population. Our biggest challenge is one of free ridership. The CDC is now asking the vaccinated to resume masking in areas of high transmission, which is now most but not all of the country. What that means is that we are again asking the vaccinated to take on the burdens of the decisions of the voluntarily unvaccinated. And that’s a big problem.
But before we get to that we need to back up and remember what the earlier de-masking guidance really was. The guidance was actually that the vaccinated could stop masking. It is generally remembered as an end to guidance to mask generally. It wasn’t. In practice though it was the unvaccinated who were quickest to stop masking if they’d ever been masking at all.
This I think was the heart of the error. The people who most benefited from masking were the least likely to follow the guidance. In the absence of a robust system of vaccine passports there was no way to distinguish one group from the other. Indeed, in much of Red State America passports have been banned even for private organizations and businesses. Basically no one payed attention to this distinction at all – and that is a problem with the initial guidance because that was fairly predictable. The emergence of the Delta variant – a new and unknown factor – just made the consequences much greater.
Today one of the most difficult things to make sense of is just how much we think the vaccinated themselves are at risk today from Delta – whether we’re defining that as infections generally or severe outcomes. One reason for the updated CDC guidance is increasing – but still tentative and uncertain – evidence that Delta COVID is spreading among the vaccinated themselves. But clearly the biggest beneficiaries of this new policy are the unvaccinated. It’s the unvaccinated among whom Delta COVID is spreading like wildfire. Infections among the vaccinated are largely spillover from that out of control situation. The unvaccinated are not only unvaccinated they are also disproportionately unmasked. (If you’re worried about COVID or trying to do your part for the larger community, let’s be honest: you’re going to get vaccinated.)
So we can see larger problem. Masking is coming back largely because of the actions of the unvaccinated and also largely for the benefit of the unvaccinated. The burden of non-vaccination is being placed on those who are vaccinated. That basic disconnect is our problem.
That disconnect places no effective pressure on the voluntarily unvaccinated while sowing demoralization and frustration and contempt with public authorities among those who’ve gotten the vaccine. No good comes of that combination. As I have been arguing, the cornerstone of our policy should focusing the burden of non-vaccination on those who are voluntarily unvaccinated. That is both the most equitable and fair approach and it is the approach most likely to increase the number of people getting vaccinated. We need to cut that cord of misplaced incentives and penalties. That’s why I think the more important and more positive developments in recent days are the moves toward mandates. We’re seeing a wave of mandates for various kinds of public employees and health care workers to get vaccinated. We’re also seeing the federal government clear the way for private organizations to do the same. That is the proper path forward. We do not need to see it as punitive. It is simply placing the burden of non-vaccination on the voluntarily unvaccinated. This is also why speeding formal FDA approval of the vaccine is so important. Despite federal court rulings that appear to give employers the right to mandate vaccines under the current emergency approval, it is clear that only that formal approval will move the mass of the employers in that direction.
One more point.
To understand the challenges with vaccinating the whole country we need to understand what the problem is. I noted Monday that while we focus most on ideological anti-vaxxers there’s a big chunk of the non-vaxed population that is more movable and less set in their decision. This chart was in Mike Allen’s Axios newsletter this morning. They’ve arranged the numbers in a confusing way. But the part I’ve highlighted tells the story.
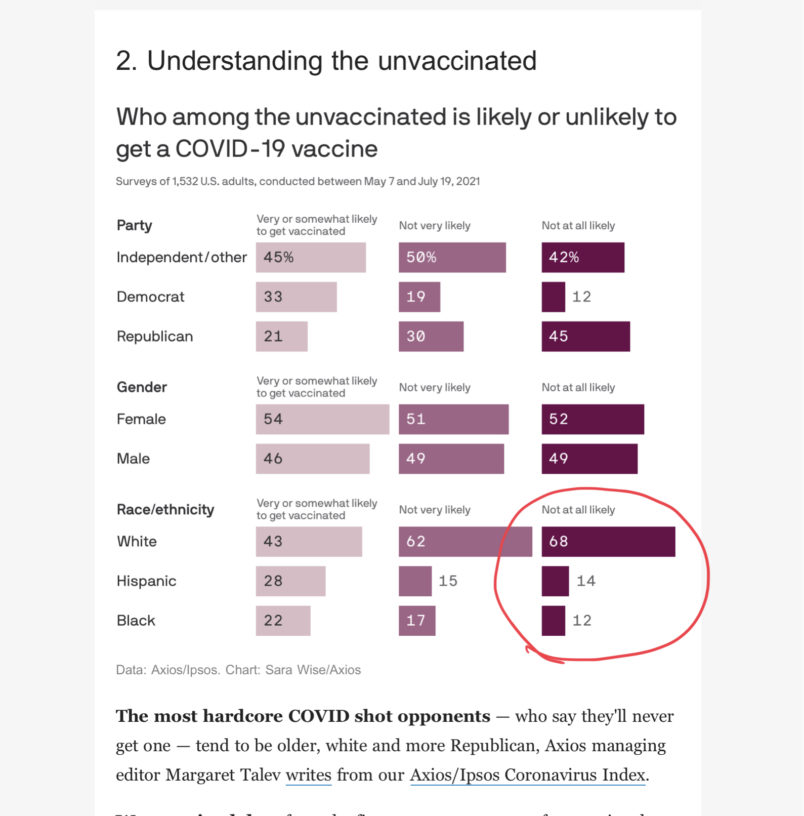
We don’t have one problem. We have two. These breakdowns show clearly that we have a hesitancy problem in the Black and Hispanic communities and a resistance problem among white Republicans. Those are different issues.
In the former case that is in part the historic experience of the African-American community and the general issue that marginalized communities are usually the hardest to vaccinate across cultures – economic private, low trust in public authorities, tenuous connection to social networks that facilitate public health efforts. That can be worked over time. The latter issue is clearly political and ideological. But for all the reasons above the best approach is not endless public discussion about understanding hesitance and resistance or persuasion. It’s mandates for vaccination. We’re not going to mandate for the whole population, though we should certainly have them for public-facing public employees and all health care workers. But in every respect we should concentrate the burden of non-vaccination on the voluntarily unvaccinated. Want to engage in non-essential indoor public activities? Get vaccinated. This is both the most equitable and most effective way forward.
Given where we are now – largely because of the voluntarily unvaccinated – some move back to public masking probably makes sense. For what it’s worth, I continue to wear a mask in public indoor settings. But our whole policy should focus on putting as little of the burden of non-vaccination on those who’ve gotten vaccinated and as much as possible on those who have not.



